Free Medical Consent Form (Template & Builder)
What is Medical Consent Form?
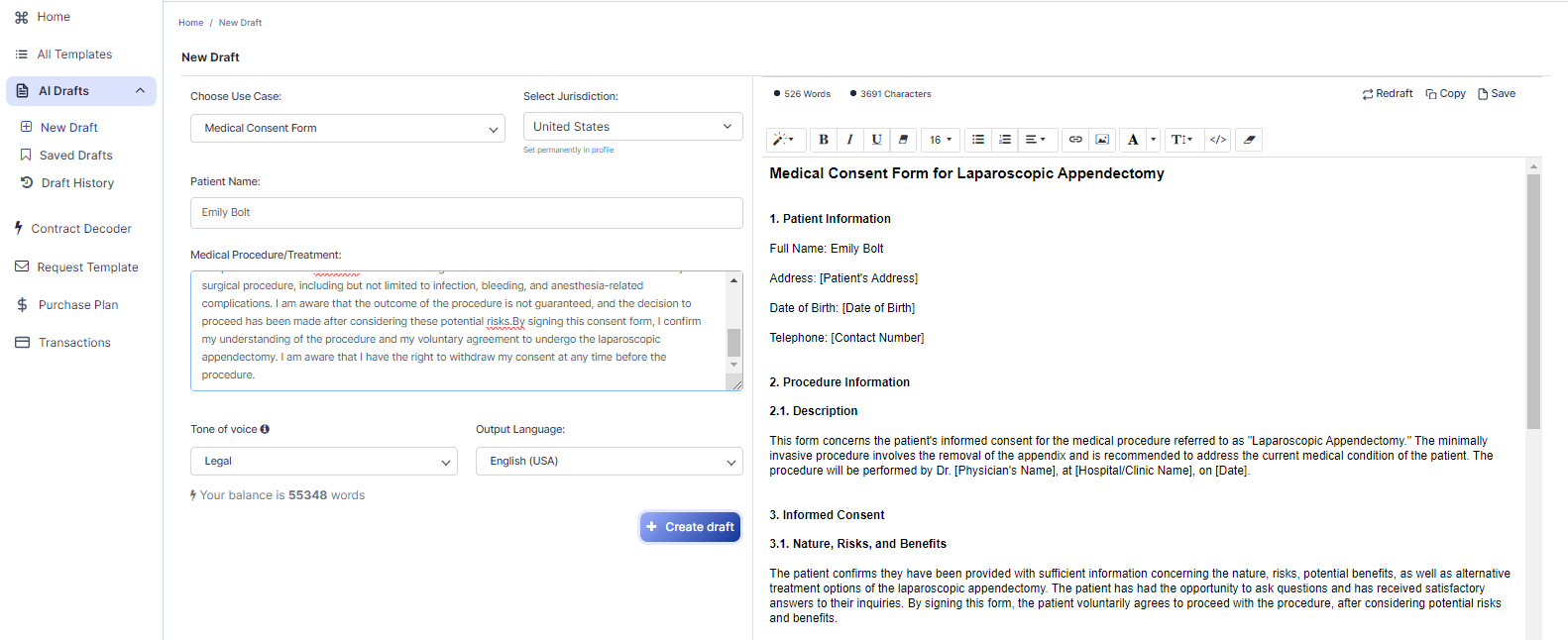
Medical Consent Form Obtains consent from a patient for medical procedures or treatment, explaining risks, benefits, alternatives, and confidentiality.
Sample template (2026):
Medical Consent Form for Laparoscopic Appendectomy
1. Patient Information
Full Name: Emily Bolt
Address: [Patient's Address]
Date of Birth: [Date of Birth]
Telephone: [Contact Number]
2. Procedure Information
2.1. Description
This form concerns the patient's informed consent for the medical procedure referred to as "Laparoscopic Appendectomy." The minimally invasive procedure involves the removal of the appendix and is recommended to address the current medical condition of the patient. The procedure will be performed by Dr. [Physician's Name], at [Hospital/Clinic Name], on [Date].
3. Informed Consent
3.1. Nature, Risks, and Benefits
The patient confirms they have been provided with sufficient information concerning the nature, risks, potential benefits, as well as alternative treatment options of the laparoscopic appendectomy. The patient has had the opportunity to ask questions and has received satisfactory answers to their inquiries. By signing this form, the patient voluntarily agrees to proceed with the procedure, after considering potential risks and benefits.
3.2. Withdrawal of Consent
The patient is aware of their right to withdraw consent at any time before the procedure is commenced.
4. Acknowledgment of Risks
The patient acknowledges the potential risks associated with any surgical procedure, including but not limited to infection, bleeding, and anesthesia-related complications. The patient has been made aware that there are no guarantees regarding the outcome of the procedure, and the decision to proceed has been made after considering these potential risks.
5. Agreement
By signing this consent form, the patient confirms they understand the nature of the laparoscopic appendectomy procedure and voluntarily agrees to undergo the treatment. If the patient is under 18 years old or incapacitated, their legal guardian or authorized representative must sign on their behalf.
6. Governing Law
This medical consent form is in compliance with the laws of the United States. Any disputes or claims arising from this consent form shall be resolved in accordance with the applicable laws of the United States.
Signature
I, Emily Bolt, confirm that I have read and understood the information provided in this Medical Consent Form. I have had the opportunity to ask questions and receive satisfactory answers from my healthcare provider, Dr. [Physician's Name]. I hereby give my informed consent to undergo the laparoscopic appendectomy procedure, after having weighed the potential risks and benefits.
Patient's Signature: ___________________________
Date: ________________________________________
If the patient is under 18 years old or incapacitated, the following information must be completed by the parent, legal guardian, or authorized representative:
Legal Guardian/Authorized Representative's Full Name: [Guardian's Full Name]
Relationship to Patient: [Relationship]
Address: [Guardian's Address]
Telephone: [Guardian's Telephone Number]
Legal Guardian/Authorized Representative's Signature: _______________________
Date: _____________________________________________
Physician's Signature: __________________________________
Date: ________________________________________________
Name (printed): Dr. [Physician's Full Name]
Address: [Physician's Address]
Telephone: [Physician's Telephone Number]
Ready to Create your own Medical Consent Form?
Common Sections of a Medical Consent Form for Laparoscopic Appendectomy
In this Medical Consent Form, you will see the following sections:
- Patient Information
- Procedure Information
- Informed Consent
- Acknowledgment of Risks
- Agreement
- Governing Law
Summary of each section:
- Patient Information : This section collects the patient's personal details, such as their full name, address, date of birth, and telephone number. It helps identify the patient and serves as a record for the medical provider.
- Procedure Information : This part explains the specific medical procedure the patient is consenting to, in this case, a laparoscopic appendectomy. It includes details about the procedure, the physician performing it, and the location and date of the surgery.
- Informed Consent : This section confirms that the patient has been given enough information about the procedure, its risks, benefits, and alternatives. It also states that the patient has had the opportunity to ask questions and received satisfactory answers. The patient can withdraw consent at any time before the procedure starts.
- Acknowledgment of Risks : The patient acknowledges the potential risks associated with the surgery, such as infection, bleeding, and anesthesia complications. They understand that there are no guarantees regarding the outcome and have decided to proceed after considering these risks.
- Agreement : By signing the form, the patient confirms their understanding of the procedure and voluntarily agrees to undergo it. If the patient is under 18 or incapacitated, a legal guardian or authorized representative must sign on their behalf.
- Governing Law : This section states that the consent form complies with the laws of the United States, and any disputes or claims arising from it will be resolved according to applicable US laws.
Ready to get started?
Create your Medical Consent Form now